

Introducing Guidelines for Intraocular Lens Exchange due to IOL Material Changes
A White Paper on Clinical Decision-Making and Surgical Management.
Introduction
Heidelberg 11 June 2026. Intraocular lens (IOL) material degradation is a cause of visual impairment and is among the primary indications for IOL exchange surgery in contemporary practice. Material changes encompass various phenomena, including calcification, glistenings, and superficial deposits, each with distinct pathophysiological mechanisms and clinical implications. (1-4) The decision to pursue IOL exchange requires careful consideration of multiple functional parameters, patient-reported outcomes, and surgical risks.
The following article arises from my own experiences in The David J Apple® Center for Vision Research and is intended to provide evidence-based recommendations for evaluating and managing IOL material changes and deposits, based on current literature and clinical experience.
Types of IOL Material Changes
Calcification
Calcification affects only hydrophilic acrylic IOLs and can be classified into primary (homogeneous) and secondary (localised) types. Primary calcification presents as a homogenous opacity throughout the IOL material, occurring months to years after uneventful surgery in otherwise healthy eyes, likely related to intrinsic material properties or manufacturing processes. Secondary calcification occurs due to external factors such as breakdown of the blood-aqueous barrier or complex or prolonged surgeries. The incidence varies widely, with higher rates in specific cohorts, particularly following endothelial keratoplasty procedures.

Image of an example of IOL calcification.
Glistenings
Glistenings represent fluid-filled microvacuoles within hydrophobic acrylic IOL materials, resulting from water accumulation in the polymers, which form pockets that enlarge with temperature changes. Different to calcification, glistenings rarely cause significant visual impairment or require explantation. The clinical impact is generally expected to be minimal compared to calcification, though severe cases may affect optical quality and increase intraocular straylight.
Anterior Surface Deposits
Surface deposits comprise a heterogeneous group of opacities located on the IOL anterior side at the IOL–aqueous interface. They can represent true material‑related phenomena (e.g. secondary IOL calcification) or secondary changes caused by altered aqueous composition in eyes with chronic uveitis, other causes of a breakdown of the blood–aqueous barrier, or intraocular hemorrhage. In contrast to material changes, these deposits typically fluctuate in density over time, depending on the underlying ocular condition and anti‑inflammatory treatment. Clinically, anterior deposits often present with increased forward light scatter and glare symptoms that may be disproportionate to the reduction in high‑contrast visual acuity, similar to other IOL material changes. Slit‑lamp examination under retroillumination and diffuse illumination, sometimes complemented by anterior segment OCT or Scheimpflug imaging, allows characterization of the location, extent, and thickness of the deposits and helps distinguish them from capsular opacification or intralenticular changes. In many cases, controlling inflammation and, where appropriate, YAG laser polishing or surgical scraping may improve symptoms without the need for IOL exchange, particularly when deposits are superficial. IOL exchange due to anterior surface deposits should therefore be reserved for patients with a clear temporal correlation between deposit formation and onset of visual complaints, morphologically relevant coverage of the pupillary area, and objective documentation of functional impairment.
Diagnostic Evaluation and Decision Criteria
Functional Assessment
Traditional reliance on corrected distance visual acuity (CDVA) alone is insufficient for decision-making in IOL material changes. Patients with IOL material changes can maintain excellent VA (20/20 Snellen) despite significant morphological opacification and vice versa. Apart from CDVA measurement, a comprehensive assessment should include:
- Morphological analysis of the opacity (e.g. by optical coherence tomography)
- Intraocular straylight assessment
- Contrast sensitivity (with and without glare)
Straylight measurement can provide an objective criterion for surgical decision-making. Evidence indicates that a straylight value above 1.56 log(s) may serve as a clinically meaningful threshold, representing the breakeven point at which patients have a 50% chance of postoperative functional improvement. (1) Values above 1.47-1.5 log(s) indicate serious straylight hindrance and may render patients unfit for driving. Following IOL exchange, straylight typically decreases, representing a clinically significant improvement.
Contrast sensitivity (CS) testing can reveal substantial deficits at all spatial frequencies, particularly pronounced under glare conditions. This reduction correlates with elevated straylight levels and may better explain patients’ subjective complaints than VA measurements alone. Post-exchange, CS typically returns to normal pseudophakic levels.
Patient-Reported Outcomes
Subjective symptoms requiring documentation include cloudy or turbid vision, decreased visual quality, increased glare sensitivity, blurred vision, and reduced contrast perception. Questionnaires provide useful tools for assessing quality-of-life impact.
Recommendations for IOL Exchange Surgery
Indications for Surgery
IOL exchange should be considered when:
- There is morphologically plausible visual impairment due to the IOL material change.
- The Straylight value is elevated, regardless of VA
- There is marked reduction in Contrast sensitivity, particularly under glare conditions
- Subjective symptoms impacting quality of life are most likely due to the IOL material change.
Relative contraindications include limited visual potential, elderly patients with limited fitness to undergo surgery and minimal symptoms/ functional impairment.
Surgical Technique and Considerations
Preservation of capsular bag integrity should be preserved whenever possible. The procedure might involve creating a superior sclero-corneal tunnel with two paracenteses, corneal endothelial protection with a dispersive Ophthalmic Viscosurgical Device (OVD), mobilisation of the opacified IOL into the anterior chamber, and explantation through the superior tunnel. Secondary IOL selection depends on remaining capsular support: capsular bag placement when adequate support remains, sulcus fixation for sufficient anterior capsular support, and retropupillary iris-claw or scleral-fixated IOL for insufficient capsular support. Anterior vitrectomy is frequently required.
Expected Outcomes
Patients undergoing IOL exchange for material changes can expect:
- Visual acuity improvement (averaging one ETDRS line)
- Substantial straylight reduction
- Restoration of normal pseudophakic contrast sensitivity
- Reduction in halo and glare phenomena
- Improvement in quality-of-life measures
Common postoperative complications include (transient) hypotonia, mild anterior chamber hemorrhage, small stromal iris defects, (transient) corneal edema and (transient) IOP elevation. Serious complications such as cystic macular edema or retinal detachment are rare.
Patient Counselling Framework
When counselling patients regarding IOL exchange for material changes, clinicians should emphasize that:
- Subjective symptoms often correlate better with straylight than visual acuity
- Success rates of IOL exchange are high with experienced surgeons
- Age alone should not determine candidacy if functional impairment can be related to the IOL material change
Depending on the pattern, localization and severity of opacity, refraining from surgery and accepting the condition can be a reasonable decision.
Conclusion
Management of IOL material changes requires a comprehensive functional assessment beyond standard visual acuity measurement. Intraocular straylight assessment provides an objective criterion for surgical decision-making. Contrast sensitivity testing and quality-of-life questionnaires complement clinical assessment. IOL exchange surgery usually yields good functional outcomes with acceptable complication rates, thereby improving vision quality and patient satisfaction.
Depending on the pattern, localization and severity of opacity, refraining from surgery and accepting the condition can be a reasonable decision.
References
- Yildirim TM, Łabuz G, Henningsen N, Son HS, Augustin VA, Britz L, Chychko L, Khoramnia R, Auffarth GU. Establishing an objective decision criterion for intraocular lens exchange due to homogeneous calcification: a prospective clinical analysis. Eye Vis (Lond). 2024 Dec 2;11(1):46.
- Märker DA, Radeck V, Barth T, Helbig H, Scherer NCD. Long-Term Outcome and Complications of IOL-Exchange. Clin Ophthalmol. 2023 Oct 31;17:3243-3248.
- Łabuz G, Knebel D, Auffarth GU, Fang H, van den Berg TJ, Yildirim TM, Son HS, Khoramnia R. Glistening Formation and Light Scattering in Six Hydrophobic-Acrylic Intraocular Lenses. Am J Ophthalmol. 2018 Dec;196:112-120.
- Auffarth GU, Brézin A, Lignereux F, Khoramnia R, Yildirim TM, Kohnen T, Bianco J. Randomized multicenter trial to assess posterior capsule opacification and glistenings in two hydrophobic acrylic intraocular lenses. Sci Rep. 2023 Feb 17;13(1):2822.
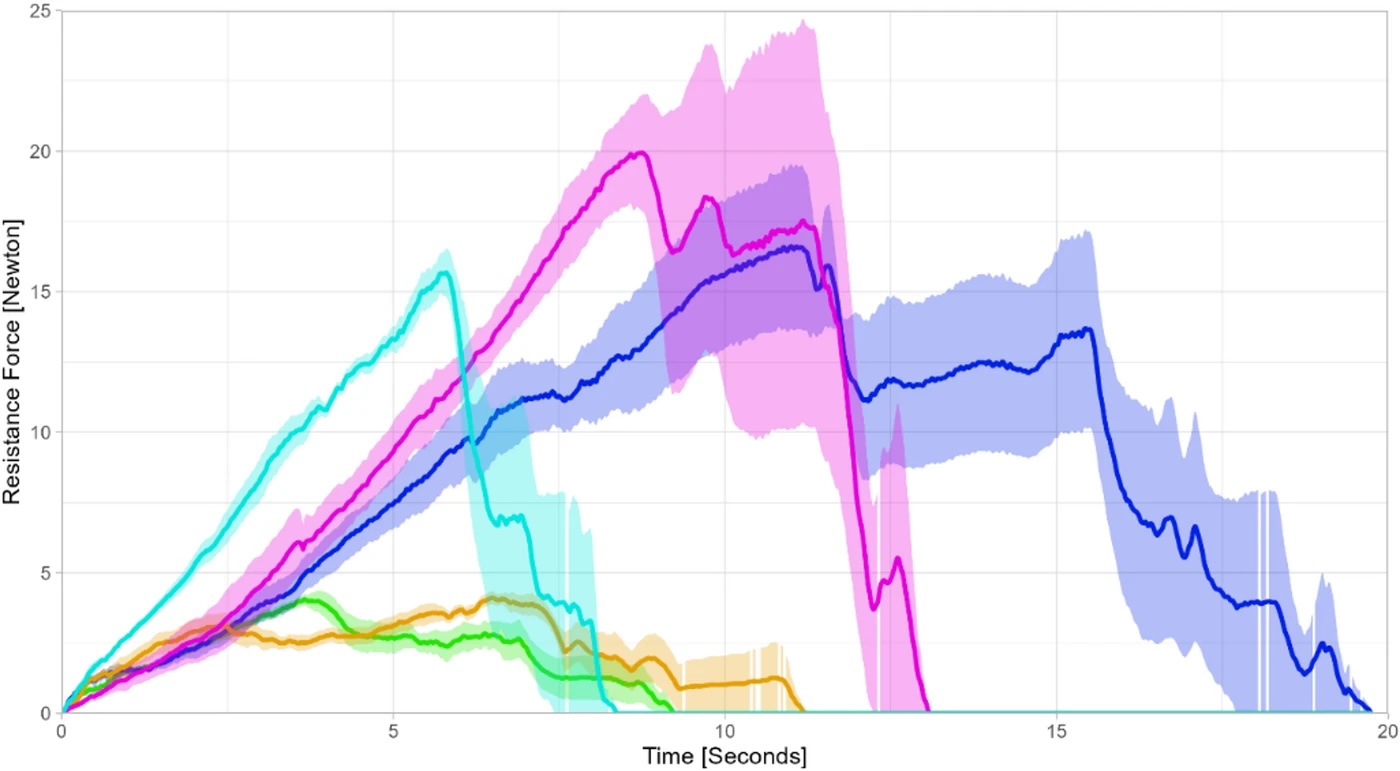 Injector Force
Injector Force