
Heidelberg, 11 May 2026. We are very pleased to report in the lastest Nature Scientific Reports, the findings of another study in the laboratory of The David J Apple® Center for Vision Research. This time, we examined the force needed to use modern intraocular lens (IOL) injectors.
Variation in resistance force during intraocular lenses injection by modern injectors and assessment of damage to the injector: a laboratory analysis.
Maximilian Friedrich, Victor A. Augustin, Donald J. Munro, Maximilian Hammer, Sonja Schickhardt, Hyeck-Soo Son & Gerd U. Auffarth
What We Did
We conducted an experimental study to help cataract surgeons select suitable intraocular lens (IOL) injectors. Our focus was on evaluating the in vitro resistance force encountered during IOL ejection and assessing the associated damage to various injector models.
How We Did It
We tested twenty-five injectors from five different manufacturers. The lenses used for injection were all +20 diopters in power. The ejections were performed into petri dishes, allowing for continuous recording of the resistance forces using an automated digital force gauge.
What Were the Results?
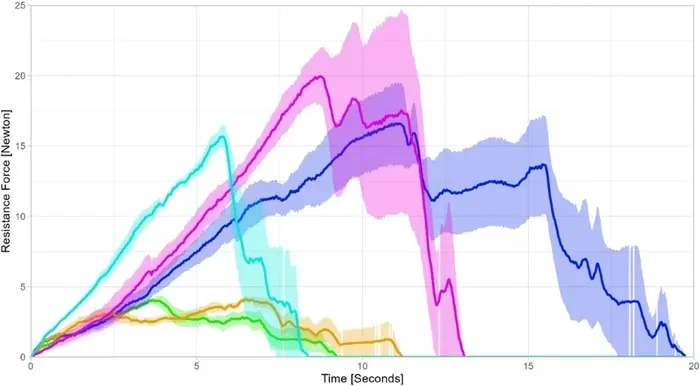
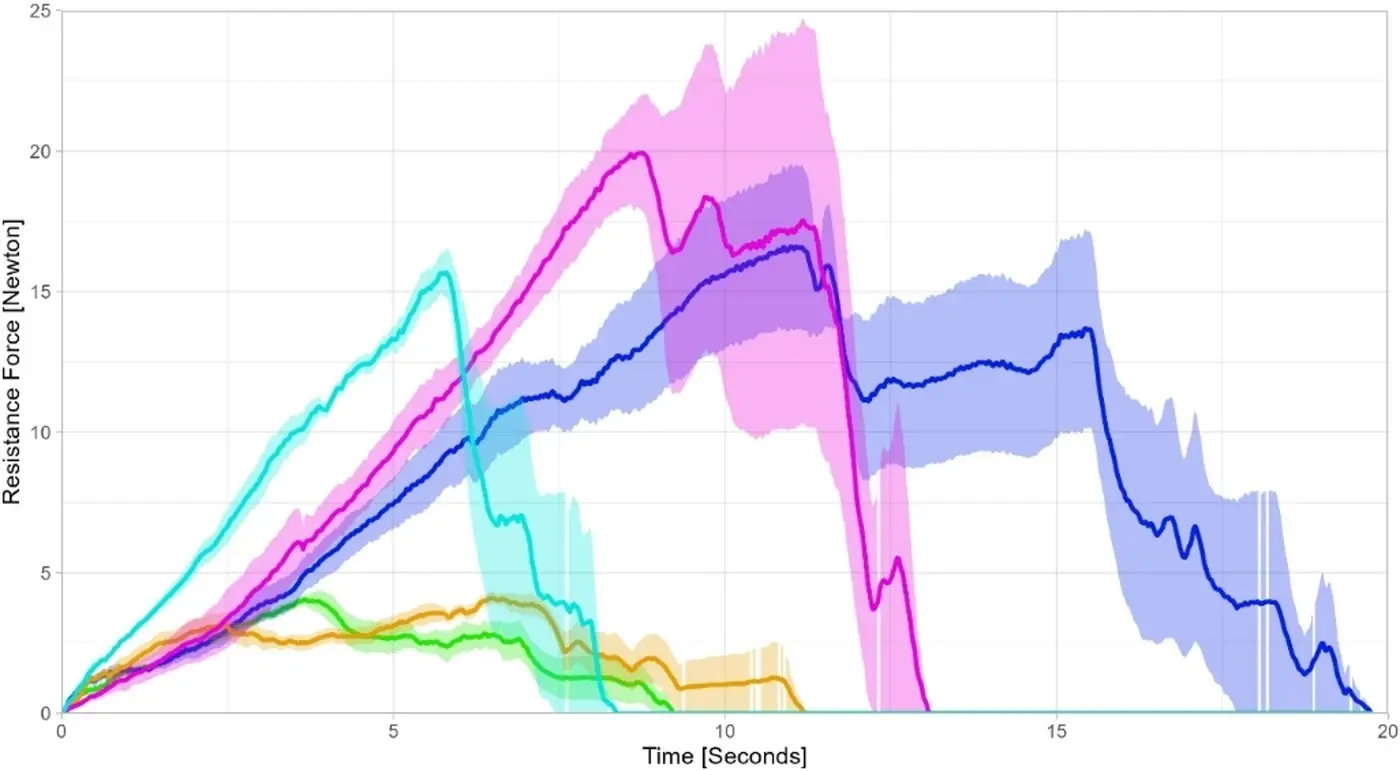
Figure 1. Overview of the mean resistance force over time during intraocular lens ejection depending on injector (*n* = 5 for each model). Shaded area: Standard error. Orange: Kowa Avansee. Blue: Zeiss Lucia. Purple: Rayner RayOne. Turquoise: Teleon Lentis Quantum & Viscoject-BIO. Green: Hoya multiSert.
We analyzed two main parameters: the maximum force exerted during ejection and the area under the curve (AUC) of the force profile.
Our results revealed significant differences in resistance forces among the injector models (p < 0.05), with maximum forces ranging from 4.39 ± 0.45 N to 25.71 ± 6.62 N.
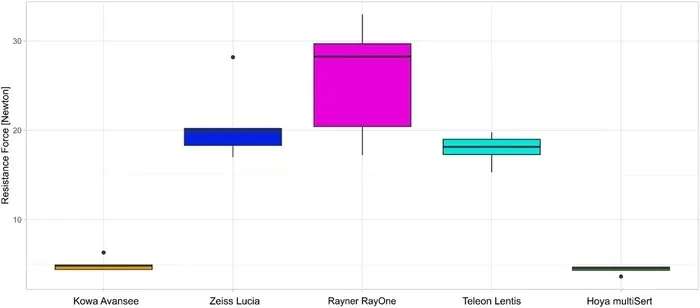
Figure 2 Area under the curve of the resistance force during intraocular lens ejection depending on injector (n = 5 for each model).
The Area Under the Curve showed considerable variability, indicating differing levels of force required for IOL delivery.
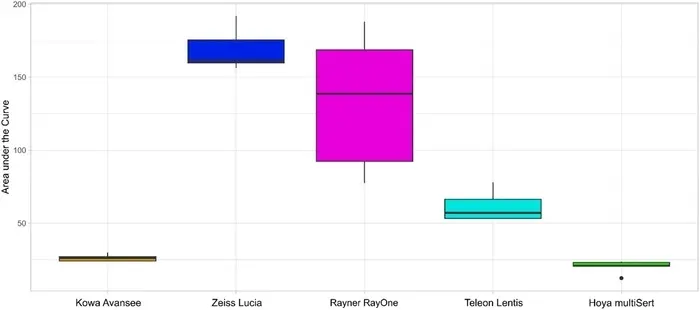
Figure 3. Maximum resistance force during intraocular lens ejection depending on injector (n = 5 for each model).
After each ejection, we examined the injector nozzle tips under a microscope and graded any damage using the HeiScore scale.
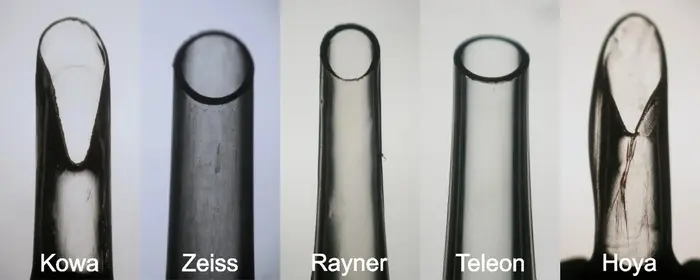
Figure 4. Example of microscopical postoperative HeiScore grading of injector nozzles.
No ejection complications were observed; however, one injector model demonstrated noticeably higher nozzle damage compared to the others.
In Conclusion
Our findings highlight the significant variability in resistance and durability among modern IOL injectors and the injectors differ in postoperative nozzle damage. Some devices allow smoother, lower-resistance IOL delivery, while others show higher force peaks or structural vulnerability of the injector tip. Surgeons shopuld recognize and expect these differences, to prevent injector-related complications intraoperatively.
Understanding these differences is crucial to ensuring safe, controlled, and efficient IOL implantation in cataract surgery. Further improvements in injector material and design may improve the resistance profile to allow a smooth and safe IOL implantation without relevant damage to the injector nozzle or the operated eye.
Our paper is open access. You can use the following link to read it in full.
 AH Cytokine and Chemokine changes after FLACS
AH Cytokine and Chemokine changes after FLACS