London, 29 November 2024. Today marks the 75th anniversary of the first IOL operation, a historic event that took place on 29 November 1949. This pioneering surgery was performed by Sir Harold Ridley, the inventor of the intraocular lens, which was made by Rayner, a company that played a crucial role in the development of the IOL.
A British surgeon, a British polymer maker and a British IOL manufacturer: Ridley, ICI and Rayner - a truly British success story.
The United Kingdom and Ireland Society for Cataract and Refractive Surgery (UKISCRS) is hosting a special congress day to commemorate the 75th anniversary of the first IOL operation. The highlight of the event is the Ridley Medal Lecture by Prof. Dr. med Gerd U Auffarth, a renowned figure in ophthalmology. In the evening, a Gala Dinner will be held at the Tower of London, organized by UKISCRS, the Ridley Eye Foundation, and Rayner. This dinner is not just a celebration, but also a fundraiser for the Foundation’s work in organizing cataract surgery camps in high altitude villages in Nepal.
What do we know about the early development of IOLs?
This is what I learned during my time at Rayner, through conversations with Harold Ridley, Ian Collins, Peter Choyce, Ernest Ford, Teddy Epstein, Eric Arnott, Piers Percival, John Pearce, and others. My notes from talking with Ian Collins and from interactions with the surgeons provides some insight into the history and development of IOLs.
Just as there is the originator of the IOL (Ridley) and then surgeon followers, (Choyce Binkhorst and Epstein) and then a later generation, (Arnott and Pearce) so too within Rayner there was a succession of champions of implant manufacture. These individuals, including John Pike, Peter Caudell, Ernest Ford, John Green, and Ian Collins, ably assisted by John Ingham, and later Peter Toop and Mike Ring. All played a crucial role in the development and production of IOLs in the first 50 years at Rayner and the transition to fodable lens production (Ring and Toop).
The batting-order from the 40s to the 90s: John Pike, Peter Caudell. Ernest Ford, John Green, Ian Collins.
Why did Ridley choose Rayner?
One might say it was destined to be because as a child Harold Ridley got his first spectacles fitted at the Reiner & Keeler shop in London. As a young surgeon in the 1930s, Rayner equipped his consulting rooms in Wimpole Street. It was during the 1930s that he met Rayner’s John Pike.
After the end of the second world war, Ridley and Pike worked on a very special project – to televise eye surgery for the first time. They would drive together to visit the Pye and Marconi electronic companies in the outskirts of London and clearly there was a trust that developed between them, sufficient for Ridley to share his plan with Pike that an implant lens could be made from plastic, not from glass.
The meeting in the car.
The story goes that Harold Ridely and John Pike discussed the secret, implant project while parked in Ridley’s Rolls in Cavendish Square. Why there? The Square is near the Rayner shop and near Ridley’s consulting rooms. I asked Nick Ridley ,why would they do that, would they be in the back together after asking the chauffeur to take a walk around the Square? Nick laughed, my father would have thought it an extravagance to employ a driver, he drove the car himself. Pike would have been in front passenger seat. The car was safe and neutral ground.
Was everyone in Rayner a supporter of IOLs?
Ernest Ford succeeded Pike and Caudell. After Ford in the 1980s came John Green and Ian Collins. These then were the IOL men inside Rayner, responsible for making IOLs, promoting lenses and making new lens designs. They worked in close contact with the surgeons. They could be distinguished from their colleagues who were more interested in the opticians shops, in spectacle-making and fitting spectacles and gemology. These colleagues were not hostile to IOLs, but for them the implants represented the “Cinderella” part of the business. We all got on well enough but IOLs was a division inside this small business.The division between the shops and the IOL business lasted well into the early 21st century, when alas, all the shops were sold or given away.
Who made the lenses?
Leonard Rofe was the man who manufactured (as in “made by hand”) the first lenses. In the 1950s and 1960s, IOL manufacture at the Rayner Optical Company was confined to one or two people only, principally Len Rofe and then his nephew John Ingham. Ian said the involvement by others in implant production was in a very low key.
Ian would add, Harold Ridley has recorded the step by step details of the first operations in his papers, but in comparision, we know little of how Rayner solved and undertook the manufacture of these first lenses. From our later knowledge we can guess, but some of the details are obscure and will probably never be known.
Who designed the lenses?
The first lens was designed by John Pike who was Rayners’ scientist in the 1930 to 1950s. He was succeeded by Peter Caudell. Pike and Caudell were both active in IOLs. Pike was more concerned with power and radius calculations and sharing with the Caudfell the increasing call for interpretting new designs of IOL. Caudell dealt more directly with surgeons and this tied in with his position of Sales Manager of the Instrument Department. Thus he attended the trade exhibitions and visited hospitals more than Pike did.
Who supplied the Perspex?
John Pike was also the link to ICI who made the Perspex material for the lens. His first contact was Dr John Holt, the chemist who, says Ridley, was contacted by John Pike sometime before 1949.
Another IC chemist J. M. J. Estevez worked closely with John Holt and took over from Holt when the he retired in the 1950’s. Estevez published Safety Requirements for Contact Lenses in the July 1966 American Journal of Ophthalmology. Estevez would have known the details that were communicated to Holt.
Ridley’s recollection that Pike consulted Holt and requested that he (ICI) produce carefully balanced PMMA containing no free monomer is incorrect. Estevez makes it clear in his article that the aircraft story prompted ICI to make available for the IOL project the pmma developed for fighter aircraft canopies. ICI did not develop a new PMMA formulation but reverted to one they had already developed in wartime for the planes.
What was the first lens like?
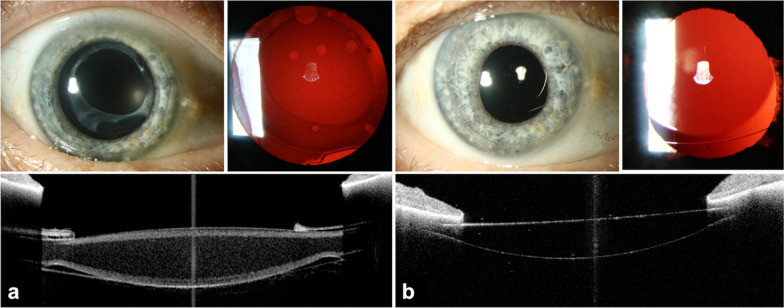
In 1949, Harold Ridley’s posterior chamber lens was 2.4mm thick which is immense when compared to today’s lenses, and its optic diameter was 8.35mm. That’s larger than today’s lens optics, although we see a tendency to approach it again. There is a groove around the circumference - used for holding the lens. The shape is well known but what is not, is that this was not in fact the design of the very first lenses Harold Ridley used. The first lens - and probably the next 25 or so -were biconvex to the edge. To hold the lens during insertion, two short grooves were filed on the surfaces of the lens. The circumferential groove was a later addition - sometime in the mid 1950s.
What were the challenges of production?
The early days of implant manufacture were very humble. The requirement was for only a few IOLs a week.
The first problem - how to generate the very short radii to give the lens its power was quickly solved. From the beginning compression-moulding was used. This was a natural choice: the polymethylmethacrylate polymers were developed by ICI to be thermo-formed, or heat-formed by compression moulding. The original material, developed during the second world war, was compression moulded to form the canopies of fighter and bomber aircraft, and optical consistency was one of the necessary properties.
We owe a debt to the polymer chemists of ICI who not only guided Rayner in setting up the process, but helped us from the start to maintain a very low level of free monomer in the material. This method produces a blank of high optical quality, and also gives a dimensional control which in some cases is still better than the modern computer-controlled lathe techniques. In the 1980s lenses were produced by lathe turning and by compression moulding for some designs.
In the production of one-piece lenses: after making the circular blank with the required optical power, the next step is to cut that blank to the required lens shape. Today companies use computer controlled engineering - or CAD-CAM. Things were not so simple in the early years - no computers then, no high precision profiling machines. To shape, or profile the lens, the blank was held on a simple piece of wood block, positioned by sight on two grooves which formed the path of the cutting disks. In this way the blank was cut to a roughly rectangular shape. The final shaping was done painstakingy and laboriously by hand filing, checking the dimensions regularly with a micrometer gauge. From these processes - crude by today’s techniques - some surprisingly intricate designs were produced.
Anterior Chamber lenses
The anterior chamber lenses from the late 1950s, Peter Choyce’s MkI, developed from the Strampelii design and the tripod AC design of Harold Ridley had flat footplates. The joint designs of Dr Jorn Boberg-Ans of Copenhagen with Mr Cogan (a consultant at Tunbridge Wells) has the Strampelli outline again, but the footplates are fenestrated - to allow greater freedom for circulation of the aqueous humour, and also to have less bulk in the anterior chamber. Another Boberg-Ans design, extends this idea and is the first of the one-piece, semi flexible anterior chamber lenses. Remarkable that these - the last two in particular - were entirely hand-crafted, shaped by hand filing. The outer edges were polished on buff wheels, checking again and again with a micrometer gauge to maintain dimensions, and by a x10 jewellers’ eyeglass to verify the finish. And the internal edges were not neglected. The lens was threaded onto silk thread and moved back and forth - back and forth until all swarf and roughness visible under x10 was removed.
On a good day, a skilled operator like Len Rofe or John Ingham could make six of these. In 1960 the Choyce MkI would have cost you 5 guineas - the Boberg semi-flexible was a little more difficult to make and would have cost you an extra guinea - 6 guineas.
And yet inspite of this labour-intensive method - or more accurately because they were all hand made, the dimensional control was excellent. Overall length -12.5mm or 13mm or whatever - was maintained to within +/- 0.1mm - much tighter than is called for in later American National Standards (ANSI) for IOLs, and the limb thickness - mainly because of the compression moulding method -was maintained to within + / - 0.05mm - 50 microns .
Where were they made?
In Brighton. Rayner did not move to nearby Hove until the 1950s.
Were they made to order?
Yes, the first lenses were packaged in a matchbox carton with a label on it with some details about the lens (style and power) and often with the patient’s name.
It is worth saying something here about the supply of lenses in 1958. Over 90% of the lenses we sold in that year were of anterior chamber design - mainly the Choyce MkI. Ian explained, the surgery was intracapsular, and almost every lens implanted was a secondary operation. A container contained six lenses. If you ordered one we sent you six - the size you required, one 0.5mm smaller, one 0.5mm larger in case your measurements were wrong - and two of each in case you dropped one. To order a lens we asked you to give us the patient’s name which we put on the container - to avoid, as Rayner’s 1960 catalogue diplomatically puts it- “to avoid any possibility of confusion in the operating theatre“ The patient’s hospital record number could also be put on the container; the affected eye, Right or Left; the spectacle refraction and back vertex distance of the spectacle lens so that we could calculate and supply the correct power; the visual acuity with correction; the refraction of the other eye and the post operative result aimed for; the corneal diameter white to white; and the type of implant required.
When the lens was implanted, the surgeon sent back the other five and Rayner credited the surgeon for these. If you sent back the container, Rayner also gave 3 guineas back for that. You got a lot for 5 guineas in 1958 - including something back on the empty bottles!
Were the lenses supplied sterile?
No, it was the surgeon’s job, or the nursing staff’s, to clean and disinfect the lens just as they ensured their metal instruments were clean for each surgery.
Cetrimide In the early years, surgeons used Cetrimide, or alkyltrimethylammonium bromide, an antiseptic. It is a mixture of three quaternary ammonium compounds: tetradonium bromide(TTAB or MITMAB), cetrimonium bromide (CTAB), and laurtrimonium bromide (DTAB or LTAB). It was first discovered and developed by ICI and they introduced under the brand name Cetavlon. It was used as a 1-3 % solution for cleaning wounds. ICI also introduced Savlon, which was a combination of cetrimide and chlorhexidine. ICI sold the Savlon brand to Johnson & Johnson in May 1992.
Caustic Soda Around 1958 sterilisation was done using sodium hydroxide - the caustic soda, or wet method. The use of sodium hydroxide as a method of sterilisation was developed in 1957 by Mr Frederick Ridley - no relation to our Harold Ridley - from a method then used for sterilising milk bottles. Using today’s definition, caustic soda treatment could never be called sterilisation - it was more accurately a method of disinfection. There was no way of proving sterility - even by sampling - since each lens was in effect treated independently. But for its time, when implant production was measured in tens of lenses instead of thousands, it worked well.
Ian Collins.
My mentor and good friend: Harold Ridley called him “young Collins”. He was Rayners’ Technical director in the 1980s, then in 1990s Managing Director. I think of Manchester: parents working in cotton mills, he was keen smoker: he started smoking in an air raid shelter, during a raid, a pupil at Manchester Grammar School. This man saw the Beatles play in the Cavern in Liverpool. He trained as an Optometrist or was it an Optician, what’s the difference I’d ask, he could be teased.
Ian first knew John Pike, as his examiner in optics. Ian would say in many of his letters and in a talk he gave at St Thomas’ Hospital in 1989, that it was of great regret to us that many of Rayner’s records dealing with the very first days of implant manufacture have been lost. Some records did remain and,when they do, they give us a picture in surprising detail. In 1958, for example, our records tell us that we supplied 255 implants. Not only do we know of what model of lens was made, and the surgeon or hospital for whom the lenses were required, but in almost every case we know the name of the patient. We know this because Ian knew it, he was the Rayner IOL historian.
Long may Rayner continue!
It was my great good luck to have worked in Rayner in the 1990s, while Harold Ridley, Teddy Epstein and Peter Choyce were still alive and I made friends with Ian Collins and David Apple. What I know about the history of IOLs I can trace to those I have named. I can talk about David on another day but today has got to be about the Rayner men (no women in this story I regret to say). They were Rayner men because they had known no other company, they started with the firm and continued until their retirement. Happy Days!
For good or for bad it is not like that today. the kind of company that Rayner was no longer exists. We can lament its passing but they still make good lenses in Worthing and good people work for Rayner.
Today, on Rayner’s special day, the 29th of November, I extend my best wishes for their continued success. May they carry on their legacy of excellence and continue to remain British!
 Flies, Blinding Worms, Spitting snakes!
Flies, Blinding Worms, Spitting snakes!