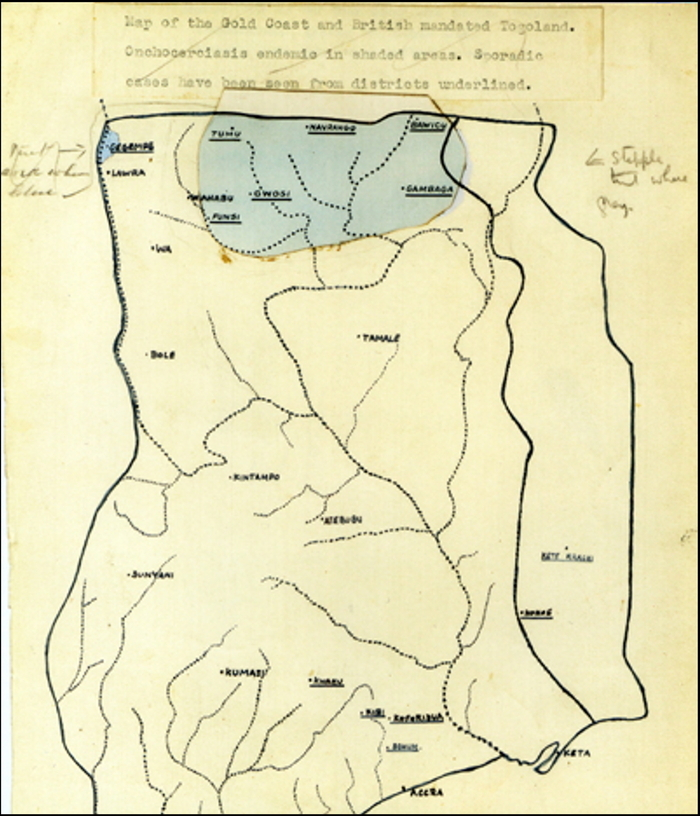
When we talk today of Harold Ridley, we recognise him for inventing and implanting the first intraocular lens. This year marks the 75th anniversary of the first lens, manufactured by Rayner in 1949. However, Ridley had other achievements in ophthalmology, apart from the IOL. Notably, in the wartime 1940s, he wrote the first detailed account in English of River Blindness - Ocular Onchocerciasis.
As we approach the anniversary date, 29th November, we will dip into the archives to learn more about Harold Ridley’s life and work.
A Novice in Tropical Ophthalmology
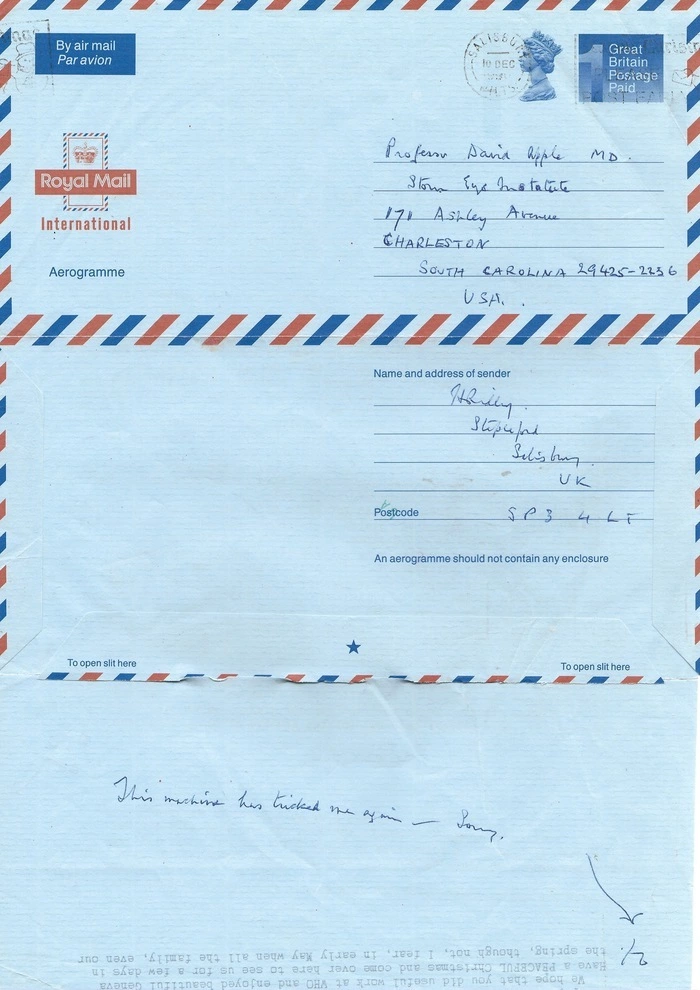
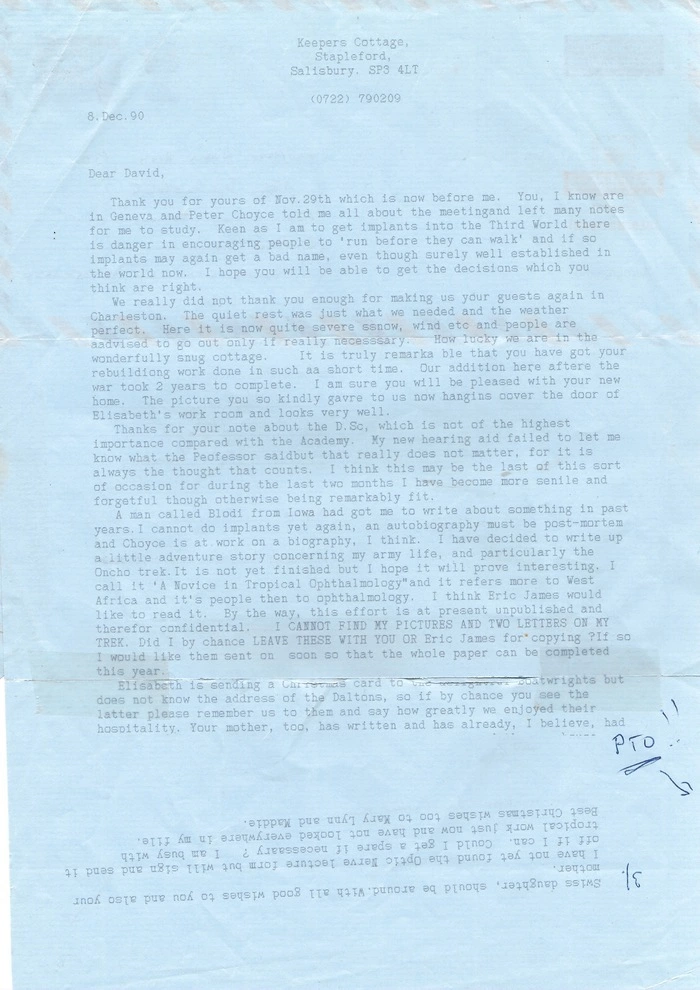
From the Archives of the David J Apple® Center for Vision Research, in a letter to David J Apple dated 8th December 1990, Ridley writes:
… I have decided to write up a little adventure story concerning my army life, and particularly the Oncho trek. It is not yet finished but I hope it will prove interesting. I call it ‘A Novice in Tropical Ophthalmology’ and it refers more to West Africa and its people than to ophthalmology. … By the way, this effort is at present unpublished and therefore confidential. I CANNOT FIND MY PICTURES AND TWO LETTERS ON MY TREK. Did I by chance LEAVE THESE WITH YOU … ? If so I would like them sent on soon so that the whole paper can be completed this year.
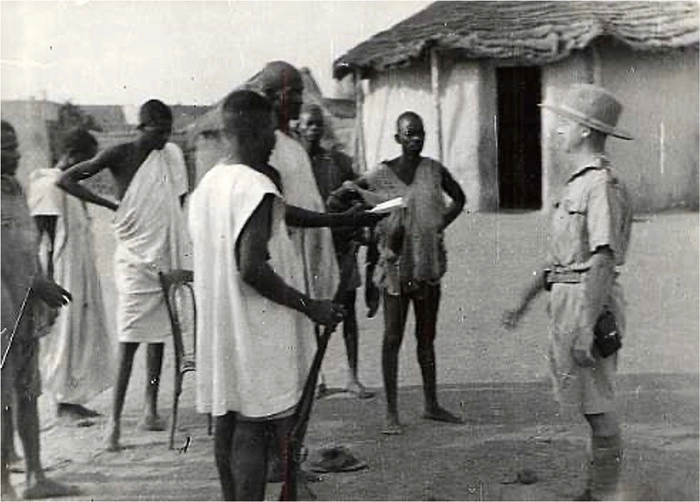
Sadly, we cannot find ‘A Novice in Tropical Ophthalmology’ among our papers. I guess that perhaps Ridley did not get far in writing it. And yes, David Apple probably did have his pictures, as several years later, in the 1996 biographical paper, (Apple DJ, Sims J. (1996) Harold Ridley and the invention of the intraocular lens.) they used the one of Ridley addressing a group of his expedition porters.
Why did Ridley go to Ghana?
It was wartime, Ridley had an order to go to West Africa
In the 1930s, Harold Ridley was a Consultant Ophthalmic Surgeon at Moorfields Eye Hospital in London. Among the other consultants was Sir Stewart Duke-Elder, who later proved to be a strong opponent of IOLs. Perhaps Duke-Elder’s hostility arose from a principled stand that Ridley had acted cavalierly by not making animal implantation studies before human implantation. But this interpretation overlooks the accounts in writing by Peter Choyce and by Eric Arnott, and in private by Ridley himself, that the two men, who had began on friendly terms, fell out with each other in the late 1930s well befroe the invention of the IOL
At the outset of the Second World War and during the Battle for Britain, both men found themselves treating fighter pilots referred to the London hospitals with ocular wounds. Ridley, while operating on these injured eyes observed that the plastic from the plane canopies was tolerated by the eye, provided the fragment was not in cntact with the iris or corneal endothelium. We do not know if Duke-Elder also noticed this but it would not be surprising if he missed it because, in general, he did not do surgery; another consultant, Sir Allen Goldsmith, operated on Duke-Elder’s patients.
After the Battle of Britain, the armed forces’ demand for ophthalmic surgery shifted outside Britain to war theatres in Asia, the Middle East, and North Africa. Ophthalmic surgeons could expect to be attached to the Royal Army Medical Corp (RAMC) as temporary commisioned officers and posted abroad to military field hospitals.
Duke-Elder had joined the RAMC in 1940, starting with the rank of lieutenant and rapidly rising to colonel, and subsequently as brigadier in the Army Medical Service he held the post of consultant ophthalmic surgeon to the Army. While he was engaged in army duties his private practice was looked after partly by his wife Phyllis and partly by Allen Goldsmith, whose general health prevented him from Army service. As the Army’s consultant ophthalmic surgeon, Duke-Elder had a role in assigning eye surgeons overseas. Harold Ridley had hoped to go to a war theatre where he could best use his surgical experience. It was a great disappointment to Ridley that he was to be “shipped out” (as he put it) to the Gold Coast (a British Crown colony in West Africa- today Ghana,) where there was no fighting. He thought it was the wish of Duke-Elder “to farm him out”. So it came about that Temp. Major Harold Ridley left England to take up the post of sanitation officer and billeted in Accra, the capital city.
The Oncho Trek
Once in Ghana, Ridley overcame his disappointment. While there is no extant account of his work on Accra’s sanitation, we do know he was not idle. He wanted to make the most of his training as a phjysician and make the best of his exile from England by studying opthalmic diseases he could only come across in Africa. We have two very fine publications from this time, one on snakebite ophthalmia (more on that in a later post) and the other on Onchocerciasis. About the latter, in his biography of Ridley, Sir Harold Ridley and His Fight for Sight: He Changed the World So that We May Better See It, David wrote.
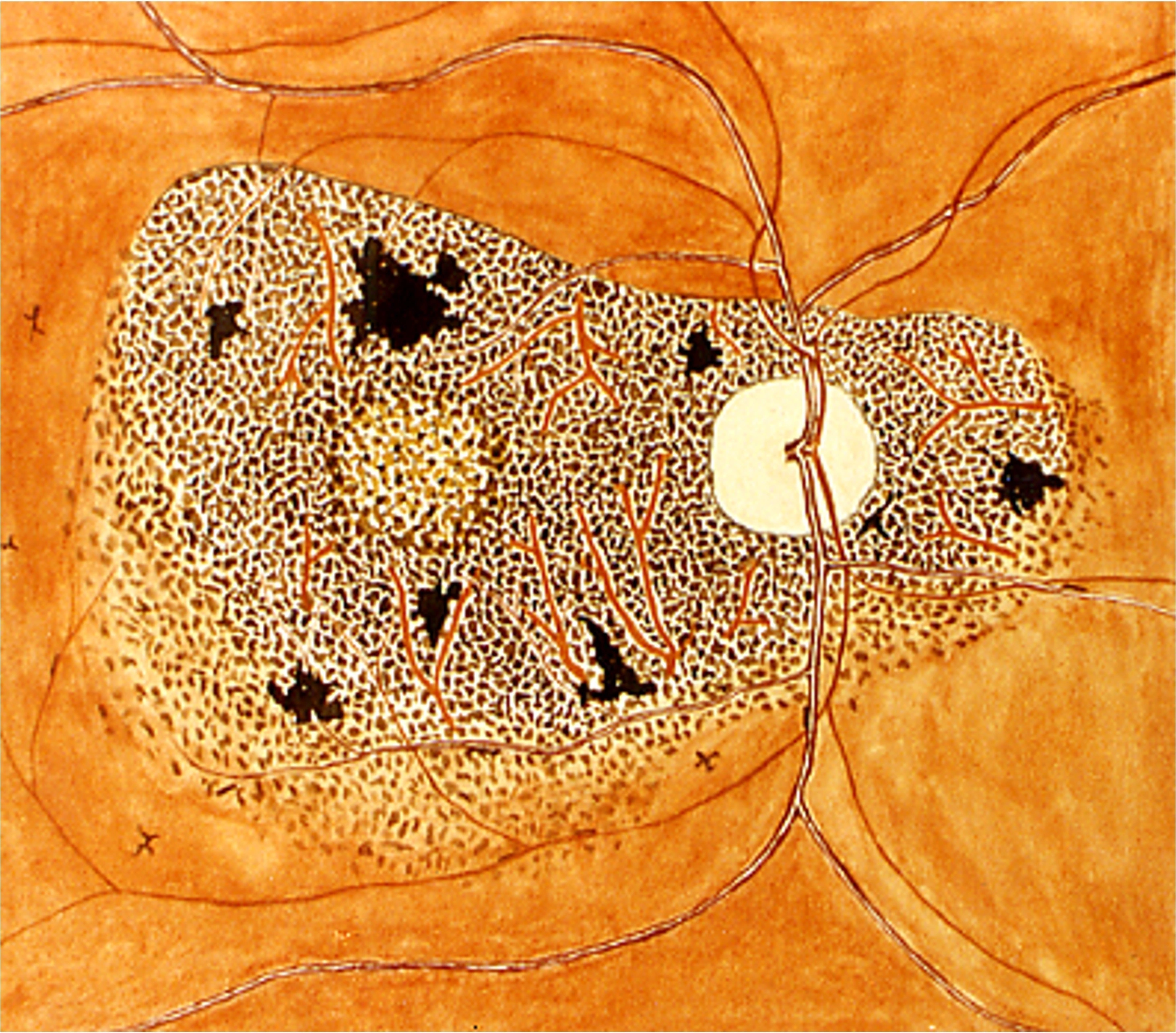
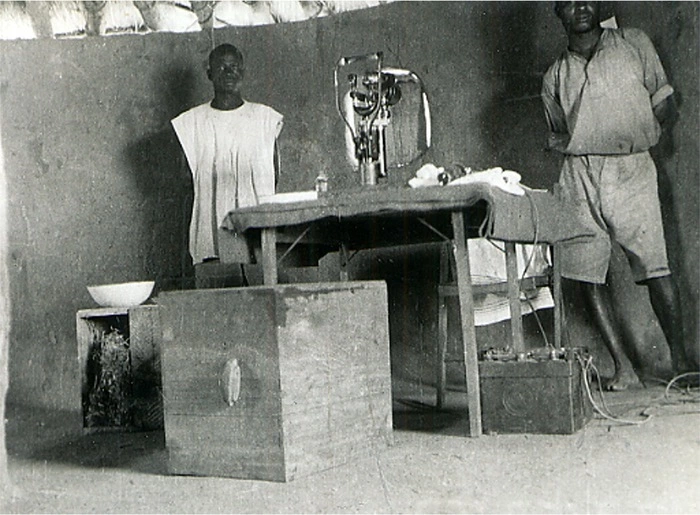
In 1941 during his war assignment in the Gold Coast (today Ghana), Ridley was appointed part-time sanitation officer and headquartered at the capital city of Accra. At that time, Ridley met Brigadier G. M. Findlay, AMS., with whom he pursued investigations on onchocerciasis. Ridley, Findlay, and Captain John Holden journeyed to Funsi, 90 minutes north of Accra*, to study onchocerciasis. They worked for two weeks, examining patients with a slit-lamp, which ran off a motor-vehicle’s 12-volt battery*. Ninety percent of the patients had onchocerciasis; ten percent of these were blind. Conditions were primitive and most of the work, even fundus painting and photography, was done by Ridley. His classic fundus painting, sometimes termed the “Ridley fundus” of onchocerciasis was completed in Accra after his return from the Bush. The attention he called to this disease constitutes one of Ridley’s major contributions. His monograph “Ocular Onchocerciasis” published in 1945 in a supplement of the British Journal of Ophthalmology was a landmark.
Unfortunately, David gives us the wrong idea about when Harold made the trip to Funsi. According to Ridley, it took place in February 1944 after being planned in 1943. There are other mistakes; Findlay did not travel with the group and David’s description of the distance between Accra and Funsi is quite wrong. One can see online that it is 488 miles / 785 km – 18 hours driving by today’s roads. Ridley writes that the slit lamp worked off two 6Volt batteries. But David’s mistakes are forgivable. He was very ill as he wrote the biography, recovering from a long period of treatments for cancer, a stroke and several bouts of pneumonia. His book was rushed out by the publisher in 2006 (Ridley’s birth centenary) - without editorial correction.
River Blindness
Funsi is a small town in the Wa district of North Ghana. The following is Harold Ridley’s own account of the trip and the work in Funsi. It is transcribed from pages 33 to 41 in his paper on Ocular Onchocerciasis.
Account of an Investigation in the Gold Coast
Application for permission to arrange a research expedition was made in July, 1943, but owing to the exigencies of the service a start was not possible until seven months later when leave became available. Meanwhile a few cases of ocular onchocerciasis had been discovered in soldiers not all of whom had inhabited or visited recognised endemic districts.
In February 1944, largely owing to the good offices of Brigadier G. M. Findlay, Consulting Physician to the West African Force, a party consisting of the writer, Captain J. R. Holden, as pathologist, and Pte. Kofi Nartey, an African Nursing Orderly as ophthalmic assistant, left Accra for the Northern Territories. One steward boy knew the Wala language and it was hoped would be useful as an interpreter, though as it turned out his knowledge was of little value. Very complete ophthalmic equipment was kindly lent by the Army Medical Services and included a slit- lamp run of two 6-volt car batteries, a projection lamp, an operating chair and instruments for ophthalmic surgery. It is believed that no slit-lamp had ever previously been taken on such an expedition and its value was unquestionable. It was necessary also to take food, drinking water and camp equipment, and it is a tribute to the country that the only firearm was a 12 bore sporting gun. Transport was provided by a 3-5 ton desert lorry.
In due course Wa, some 500 miles inland was reached, not without delays due to roadblocks caused by fallen trees and broken culverts. Dr. Maurice Browne, the Colonial Medical Service Officer, entertained the party and put at its disposal his local knowledge which was of the greatest value since those on the expedition had but slight knowledge of local bush conditions. At the time he was strenuously engaged with an epidemic of cerebro-spinal meningitis in addition to the usual diseases such as trypanosomiasis, malaria, yaws, schistosomiasis, and dracontiasis, all of which are very common. Captain Holden was able to assist in controlling an outbreak of anthrax.
It was soon decided that though the main roads were just passable to a loaded 3 ton lorry there was no chance of negotiating bush roads, the surface of which is at the best laterite and the width sometimes only the bare track of a car and bordered by a deep ditch to provide drainage in the heavy rains. Such roads are impassable to all wheeled traffic during the rainy season. Every few hundred yards there are culverts composed only of bush sticks covered with laterite, never very strong structures and towards the end of the dry season so weakened by white ants that they frequently give way beneath the weight of a car; dozens indeed did so. In view of transport difficulties a search was made in relatively accessible villages near the Black Volta but no onchocerciasis was found although trachoma and pterygium were common. It was decided therefore to adhere to the original idea of visiting Funsi, some 40miles direct, but 64 by road from Wa.’ At the last moment Dr. Browne most kindly offered to convey the party with minimal equipment to Wahabu on the river Kulp- wan whence a trek of some 12 miles would lead to Funsi. In actual fact despite difficulties it was found possible to drive right through, crossing the river by ford. On the return journey, however, the car ran off the road owing to a collapsing culvert, breaking a spring and damaging the steering. To save weight, much equipment was left behind at Wa. Only one steward boy was taken on and the medical equipment reduced to the slit-lamp, the projection lamp, a few operating instruments and essential drugs. Food consisted of five small loaves and a few tins of canned food. Twelve petrol tins of drinking water were carried and were just sufficient with care to last a week. The whole made up14 head loads varying from 20 to 68lbs.each. The 12bore and a borrowed express rifle were relied upon to augment the food supply for little, if anything, could be obtained from the villagers who had nothing to spare.
It is evident that for a complete survey a far more elaborate expedition is required. Further medical assistance as well as the services of an entomologist and a skilled photographer would have been of great value and the shortage of time imposed severe limitations. A highly organised and costly expedition of this type would require adequate transport and a regular supply of fresh food and most important of all, water. It is to be hoped that at some future date the subject of onchocerciasis in Africa will attract the attention of a research organisation.
Conditions at Funsi. The country and the people. The village stands on high ground in savannah country outwardly resembling Dartmoor in August; scorched grassland with granite outcrops and few trees except beside the water courses. The harmattan, the hot arid wind from the Sahara was in season and the small streams were completely dried up.
The village is composed of mud huts and the people are said to number 500-700. The nearest inhabited area is some 15 miles away, Wahabu having been deserted for some reason not ascertained. The inhabitants are Sissalas, members of a small tribe, with a language of its own. They are exceedingly poor for the land is infertile, producing little except guinea corn and yams and those in very moderate quantities. These products together with shea butter made from the nut of a local tree, a certain amount of game and a little river fish comprise the food supply. Game is hunted with bows and arrows, and fish caught with hook and line or by poisoning pools in the dry season with a cultivated-plant called “biel.” The appearance of the inhabitants suggested considerable malnutrition; the last harvest had been poor and there was undoubtedly a deficiency of vitamin A which is practically absent from shea butter. The only iron implements are knives and arrowheads. The women’s clothing consists of a tail of leaves fore-and aft attached to a girdle round the waist and the men wear a sort of triangle of hide-and a leather sling over the shoulder to carry a quiver. The chief and some of the wealthier people have cotton clothes. The heads of both sexes are completely shaved, a custom which rendered examination for head nodules simple. The women are degraded and of lower mentality than the men, but their duties require little intelligence; they are the “hewers of wood and drawers of water” carrying large calabashes on their heads from surface wells or sometimes from the big river 5 or 6 miles away. Tiny children are usually strapped to the backs of the women so that even in infancy there is risk of infection with the onchocerca. Marriage seldom occurs before the age of 20, but morality is of a high standard, venereal disease being very rare though exceedingly prevalent in more civilised areas. There is good reason to believe that syphilis is unknown. Polygamy is, however, the custom, the chief having 9 wives. Infant mortality is around 15 per cent. compared with 50 per cent. further south. Trypanosomiasis and malaria were said to be relatively uncommon and were it not for the eye disease the district might be relatively healthy.
Despite their many hardships the Sissalas are nature’s gentlemen. The chief was most friendly and helpful and never failed to pay an official call with his retinue at the end of the day to render thanks for work done. His people were happy, agreeable and honest. Instruments, medicines, clothing and even guns could not be guarded constantly yet not a single article was lost, though the average income must have been a few shillings per annum and the present of even an empty sardine tin was received with grateful thanks. The chief refunded the money paid for the one purchase of yams and provided eggs when he had any, and the larger of two fish caught was offered as a present. Though food is nearly always scarce no one starves for they help each other. Were it not for this there would be little hope for the blind who are an economic loss to the community. Surely such people deserve assistance to rid them of blindness, their chief scourge.
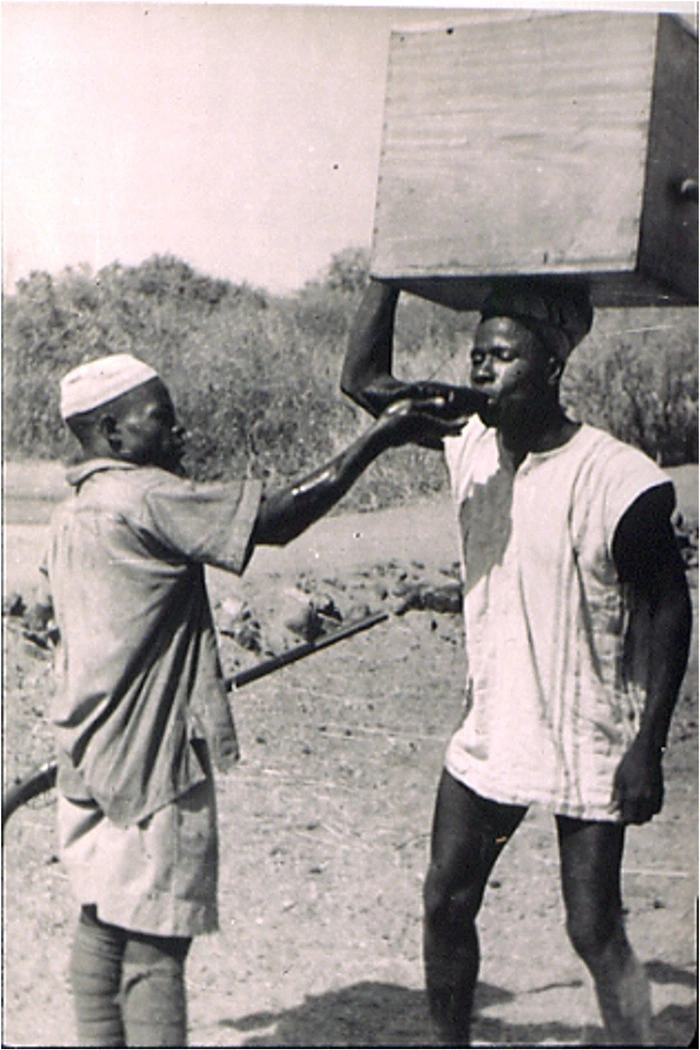
On departure, with mutual regret, presents were exchanged, and bearers provided to carry the equipment to Wahabu. Some were surprised by the weight of the accumulators, but the 12 miles were covered in 3hours. The man with the slit-lamp weighing 68lbs never left the party by 10 yards, he had been warned of its value and evidently attributed much “ ju-ju” to it. Electric light, of course, had never been seen before and, indeed, years may pass without the visit of a single white man. Fortunately two Sissalas spoke English and were invaluable as interpreters. They were intelligent men and explained the local customs and conditions. They said that the people recognised the importance of head nodules, which they called” Nukoli,”as a cause of blindness but attributed no harm to “Sangeli” nodules on the trunk. Two persons had visited a native surgeon at Belepong, the next village, to have head nodules excised, but most feared the native doctor.
Medical examination of the people. A dark room was set, up in a mud hut, the small windows of which were darkened by interested spectators, and after demonstrations on Europeans foIlowed by the chief and other influential persons the populace readily submitted to examination. It was hoped that the entire population would be examined but limitations of time prevented this and only some 300 were seen, a number comprising perhaps an unduly high proportion of eye cases. A higher proportionof those with poor sight attended on the first days but on the other’ generally failed to appear owing to fear or to engagement with domestic duties, and it was said that there were several aged and infirm, blind persons who could not easily be moved. It is possible therefore that the figures for the proportion of the population with defective sight may be more accurate than are claimed. One hundred and thirty-one persons were examined with the slit-lamp and ophthalmoscope, and of these 61 had serious eye disease, 51 ocular onchocerciases including 22 who were below British-blind certification standards, and 11trachoma. Signs of vitamin A deficiency were practically universal. These figures compare with those of Larumbe (1928) -who reported from Mexico 800 eye patients, including 100 blind amongst 4,000 persons with onchocerca nodules. Hisette(1931) at Sankuru in the Belgian Congo found that 50 per cent. of those with nodules had eye lesions, 10 per cent. being blind, Strong (1931) in Guatemala 54 ‘per cent., and Hawking (1939) at Kakamega in Kenya 34 per cent.
At Funsi many factors rendered ophthalmic examination difficult, particularly with the slit-lamp, and doubtless some points, escaped notice which would have been apparent in normal circumstances. In one important respect the expedition was a failure, for no blind eye was excised. The disease though painful in the later stages is not excruciating and the Native Administration Clerk said that it was believed that if an eye was taken from a man his soul passed to the recipient so that even a post-mortem would be refused. The offer of a glass eye or the writer’s own spectacles failed to overcome the tribal beliefs. Hisette (1932) encountered similar difficulty. The lack of pathological material ‘imposes a severe limitation on this investigation. Captain Holden did much to augment the popularity of the visit by excising 40 nodules, chiefly from children, under local anaesthesia. He also confirmed the diagnosis in doubtful cases by finding microfilariae in conjunctival snips and made several permanent microscopical specimens.
From this, the reader can see that not only was Harold an accomplished surgeon inventor and scholar but he could write well and succinctly about his work. I have never been to Funsi but I have walked on Dartmoor: I get the picture.

Roadblock
Harold was fond of an anecdote he omitted from his written account. I heard it too from Nic, Harold’s oldest son. Not long after leaving Accra, there was indeed a roadblock caused by a fallen tree so great in size they could not drive over it or get around it. They got out of the lorry, and, being British, someone made tea while they talked about what they might do, given that they had no axes, no saws. The tree’s girth was such that they could not see over it, but after a while, they could hear noises, the sound of a motor approaching and, later, voices. Ridley called out and learned from the reply that this was a British army group in the same predicament but on its way south, going to Accra. They had a similarly sized lorry. So, the parties agreed that they would change places and swap vehicles. Ridley’s group moved the slit lamp and all of their gear from the lorry on the south side to walk around the tree to the lorry on the north side. Thus, they drove on to their destination.
Monograph
“Ocular Onchocerciasis” was published in 1945 in a supplement of the British Journal of Ophthalmology. We are fortunate to have Sir Harold’s own copy which he gave to David. A full pdf of the paper will be made available in a future post on this website.

Further Reading
Apple DJ, Sims J. Harold Ridley and the invention of the intraocular lens. Surv Ophthalmol. 1996 Jan-Feb;40(4):279-92. doi: 10.1016/s0039-6257(96)82003-0. PMID: 8658339.
David J. Apple. (2006) Sir Harold Ridley and His Fight for Sight: He Changed the World So that We May Better See It. Thorofare, NJ: Slack Inc. ISBN 978-1-55642-786-2
Auffarth GU, Schmidbauer J, Apple DJ. Zum Lebenswerk von Sir Nicholas Harold Lloyd Ridley \[The life work of Sir Nicholas Harold Lloyd Ridley]. Ophthalmologe. 2001 Nov;98(11):1012-6. German. doi: 10.1007/s003470170019. PMID: 11729731.
 Fine by name and by nature
Fine by name and by nature